![]()
(potassium citrate/potassium hydrogen carbonate)
8 mEq and 24 mEq prolonged-release granules


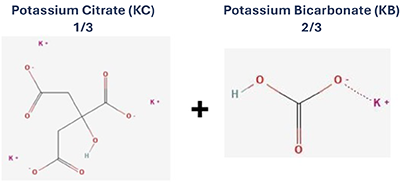
Bicarbonate and Citrate
Provides alkalizing effect necessary to buffer the metabolic acidosis
Citrate
Corrects hypocitraturia. Also acts as a calcium chelating agent reducing calcium salt crystallisation which could lead to nephrocalcinosis and nephrolithiasis
Potassium
Corrects hypokalaemia to help avoid muscle weakness and cardiac disorders
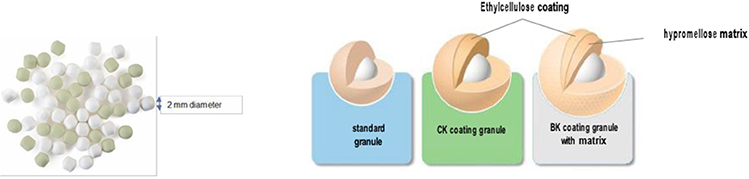
Granules
- Suitable for achieving prolonged-release oral formulation
- Two-millimeters diameter, favourable size for acceptance in young children/infants
- Two colours: green granules (potassium citrate) and white granules (potassium bicarbonate)
Coating
- With a polymer coating offering a versatile diffusion barrier. Coating thickness appropriately chosen
- Ensures taste masking and good palatability
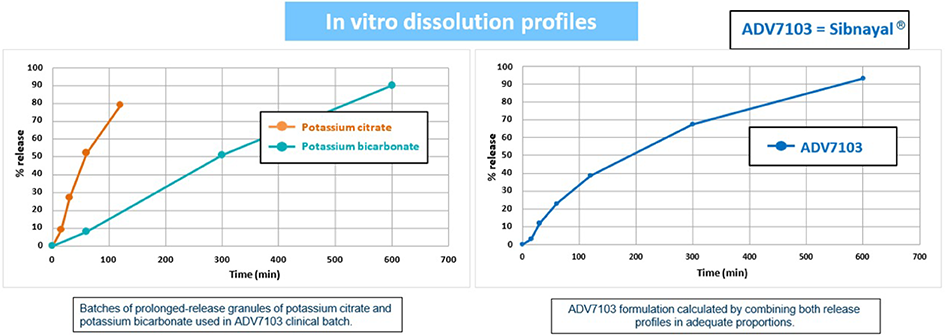
Prolonged release
- Straightforward option to reduce the number of intakes and maintain activity for an extended period (day & night)
- Provides good gastro-intestinal tolerability by limiting the alkaline load in the stomach
Potassium Citrate is absorbed from the upper part of the intestinal tract while Potassium Bicarbonate is absorbed throughout the digestive tract
Bertholet-Thomas A et al.2021. Pediatric Nephrology.36:83-91
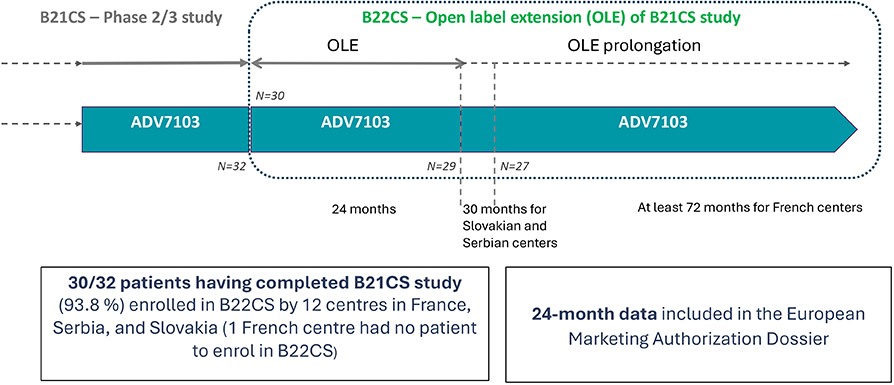
- Design: multicentre, open-label, non-inferiority, sequential, phase 2/3 study to compare ADV7103 to SoC in dRTA patients
- Aim of the study: to evaluate short-term efficacy, acceptability, tolerability, and safety of ADV7103 in comparison to SoC in adult and paediatric dRTA patients
- Inclusion criteria: males or females, aged 6 months-55 years old, with acquired or inherited dRTA, treated with SoC
- Exclusion criteria: additional proximal tubular signs, hyperkalaemia (plasma potassium >5.0 mmol/L, moderate or severe kidney impairment (GFR <45mL/min/1.73m2), patients receiving potassium-sparing diuretics, angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists, or tacrolimus
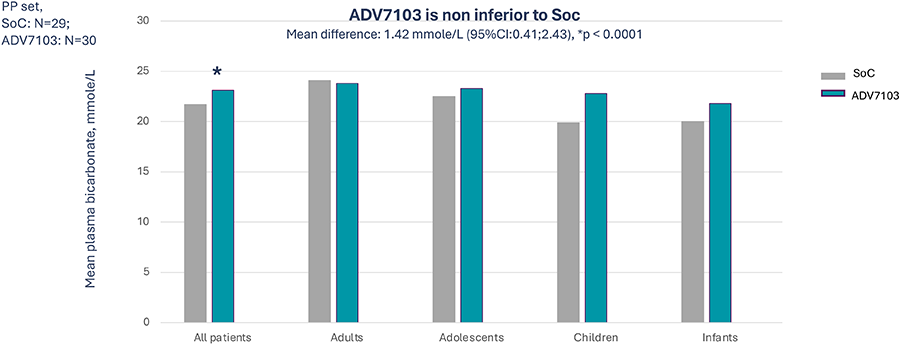
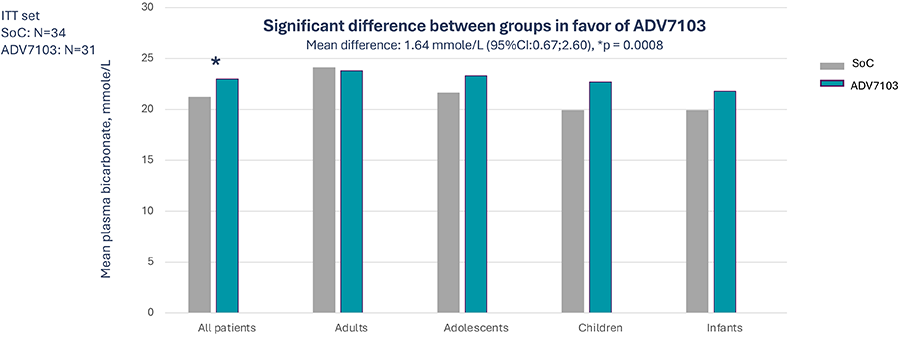
- Primary objective: efficacy on metabolic acidosis measured by bicarbonatemia
- Secondary objectives: efficacy on hypokelemia and renal markers, palatability and acceptability, safety and tolerability
- 37 dRTA patient enrolled in 13 centres across France, Serbia and Slovakia
- Inherited dRTA= 36
- Acquired dRTA (Sjögren syndrome) =1
Primary endpoint: Mean pre-morning dose level of plasma bicarbonate over 3 consecutive days (D2 to D4) at alkali steady state (Period 1 vs Period 3)
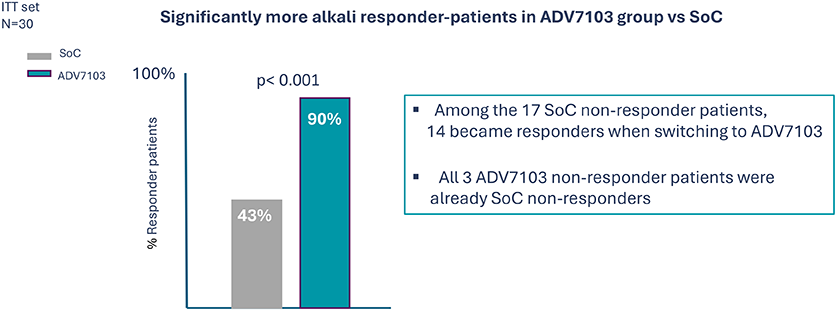
Secondary endpoint: % alkali responder for mean bicarbonate values (all bicarb normal values) over 3 consecutive days (D2 to D4) at alkali steady state (Period 1 vs Period 3)
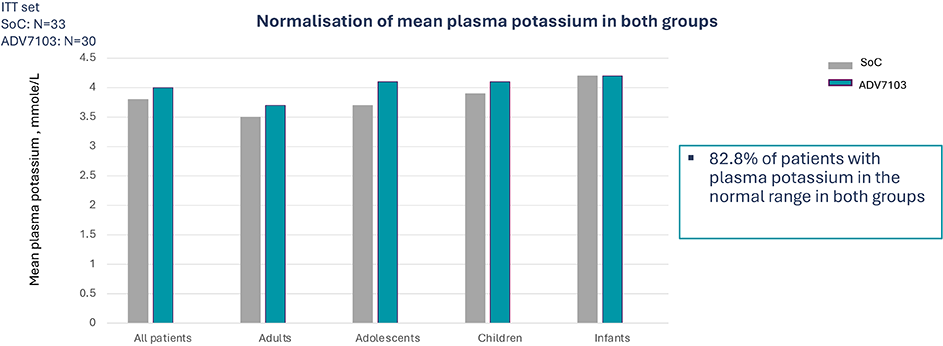
Secondary endpoint: Mean pre-morning dose level of plasma potassium over 3 consecutive days (D2 to D4) at alkali steady state (Period 1 vs Period 3)
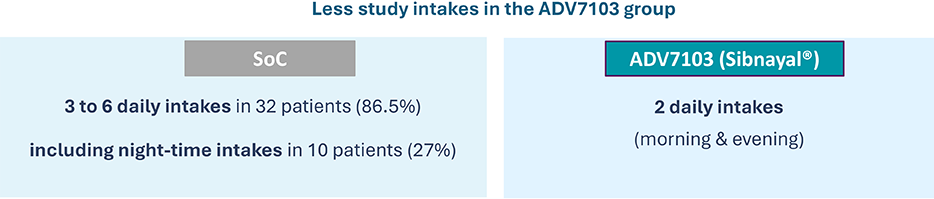
Secondary endpoint: Number of alkali treatment daily intakes (Period 1 vs Period 3)
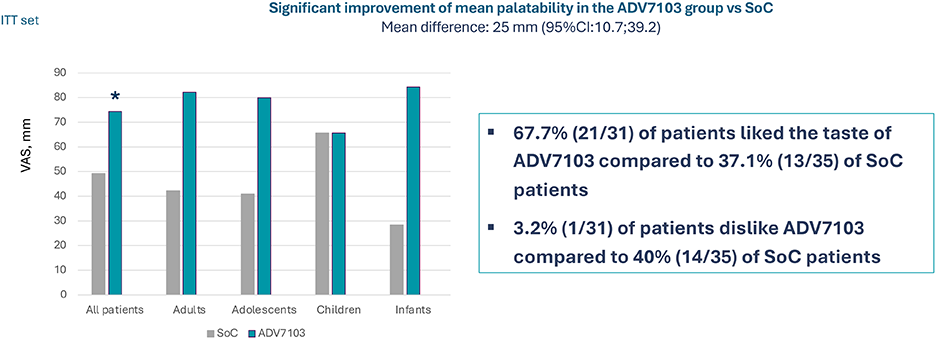
Secondary endpoint: Acceptability / Alkali palatability, VAS from 0 (dislike very much) to 100 (like very much), Period 1 vs Period 3
Secondary endpoint: Tolerability Profile (1)
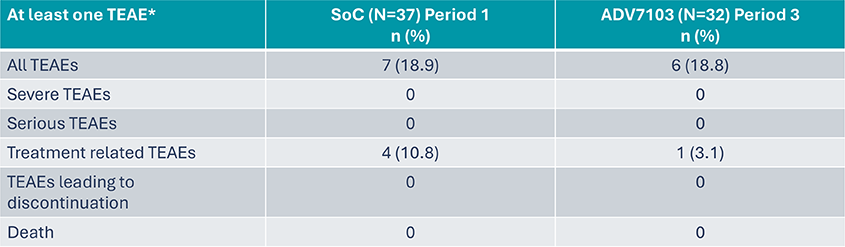
*TEAE: Treatment Emergent Adverse Event
Secondary endpoint: Tolerability Profile (2)
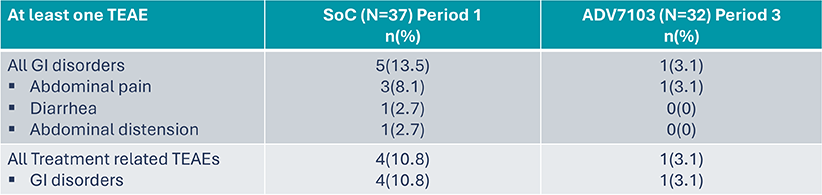
*TEAE: Treatment Emergent Adverse Event
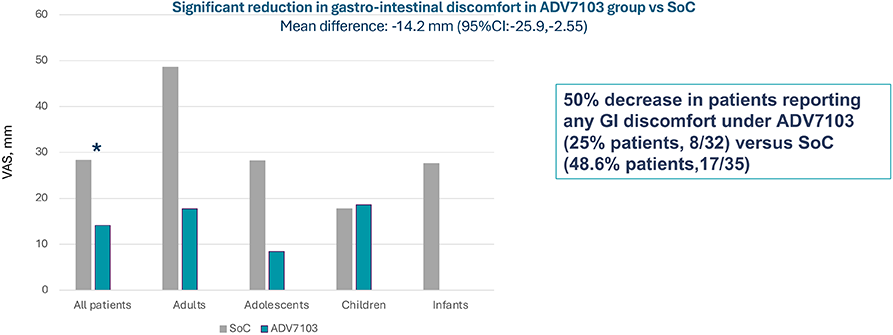
Secondary endpoint: Gastro-intestinal discomfort, VAS from 0 (no complaint) to 100 (extremely severe complaint), Period 1 vs Period 3
Primary endpoint: Number/percentage of patients presenting at least one TEAE*
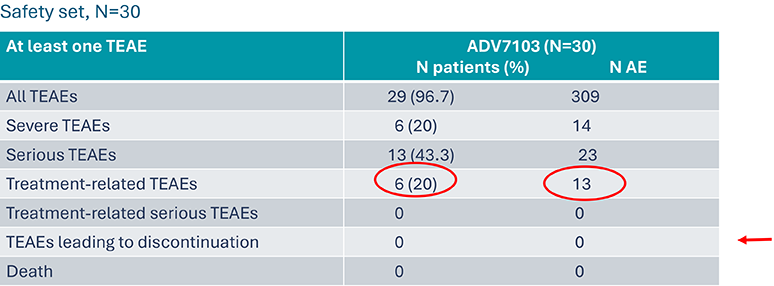
13 related TEAEs and resolved without treatment discontinuation. They concerned 6 patients (20%):
- 11 were gastro-intestinal
- 3 diarrhea in one patient
- 2 abdominal pain in two children
- 2 dyspepsia
- 2 upper abdominal pain
- 1 gastro-intestinal disorder in one adolescent (required dose adjustment with no consequence on plasma and urine metabolic parameters)
- 1 gastro-intestinal pain
- 1 hypokalemia (1 patient)
- 1 nephrolithiasis (1 patient)
No hyperkalemia
*TEAE: Treatment Emergent Adverse Event
Secondary endpoint: Treatment compliance (according to retrieved study drug), % pts
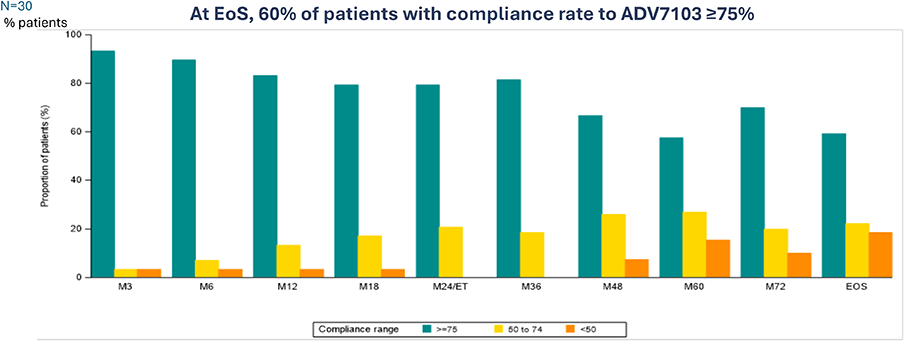
*End of Study: last study visit of B22CS
Secondary endpoint: Mean plasma bicarbonate level
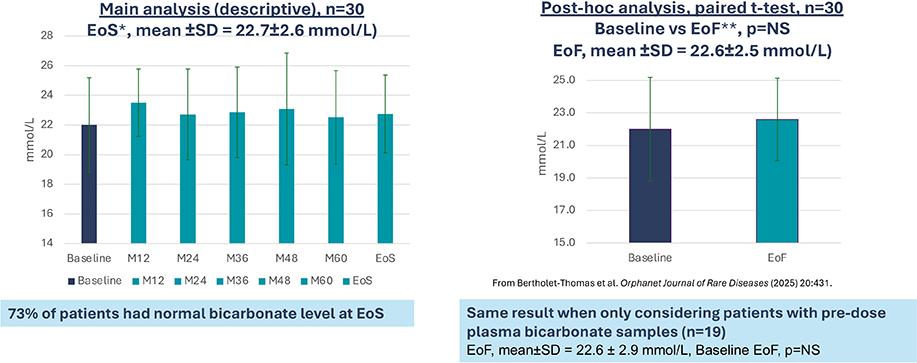
*End of Study: last study visit of B22CS
**End of Follow-up : last follow-up data available in B22CS
Secondary endpoint: Mean plasma potassium level
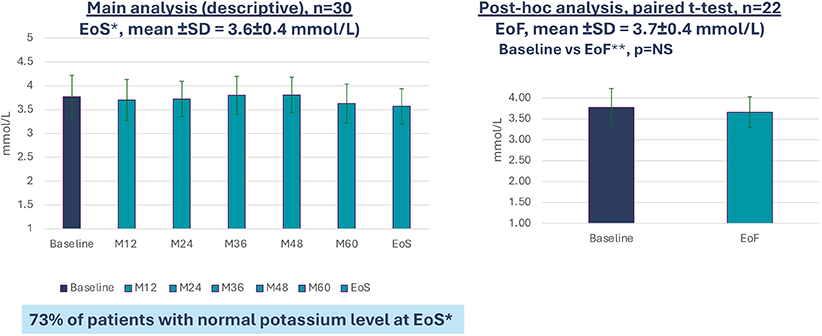
*End of Study
**EoF : End of Follow-up : last follow-up data available in B22CS.
Secondary endpoint: Mean eGFR (CKiDU-25) and KDIGO CKD stages breakdown
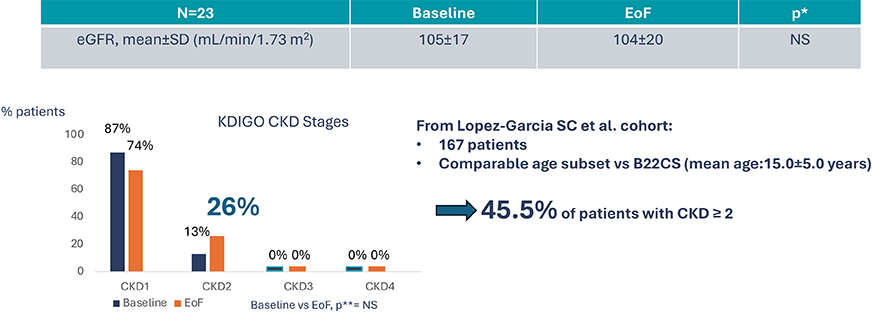
*Post-hoc analysis, paired t-test
**Post hoc analysis, Mc Nemar test
Exploratory criteria: Height
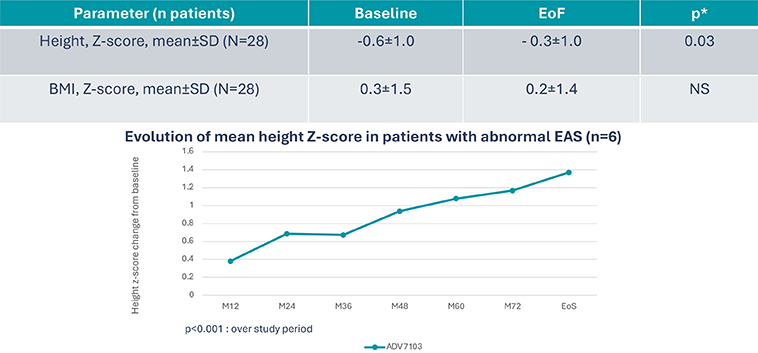
*Post hoc analysis, paired t-test
Exploratory endpoints: urinary ratios, crystalluria, nephrolithiasis, nephrocalcinosis

- % patients with positive crystalluria tended to decrease: 53% at baseline vs 35% at EoF, p*=NS
- 70% of patients with UpH between 7-8 (Baseline and EoF)
- No impact on ACCP crystals presence when UpH was > 8 (ACCP: 47% of patients at inclusion versus 35% at EoF, p*=NS)
- Nephrolithiasis: 21% of patients at Baseline vs 44% at EoS
- Nephrocalcinosis: 86% of patients at Baseline vs 92% at EoS
*Post hoc analysis, mac Nemar’s test
ACCP: Amorphous Carbonated Calcium Phosphate
Exploratory endpoints: Bone metabolism parameters
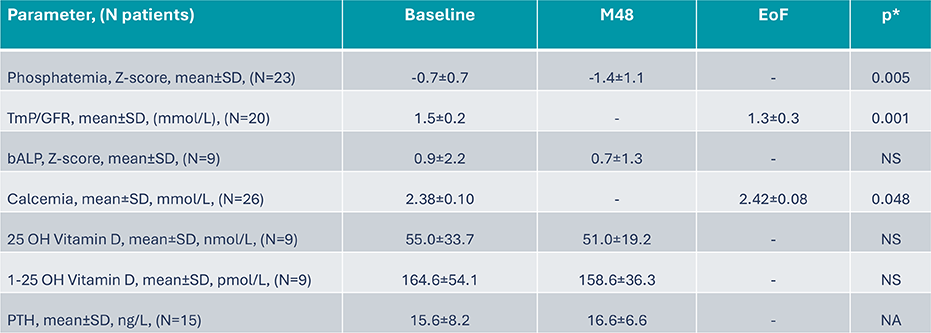
*Post hoc analysis, paired t-test
Exploratory endpoints: Lumbar Bone Mineral Density
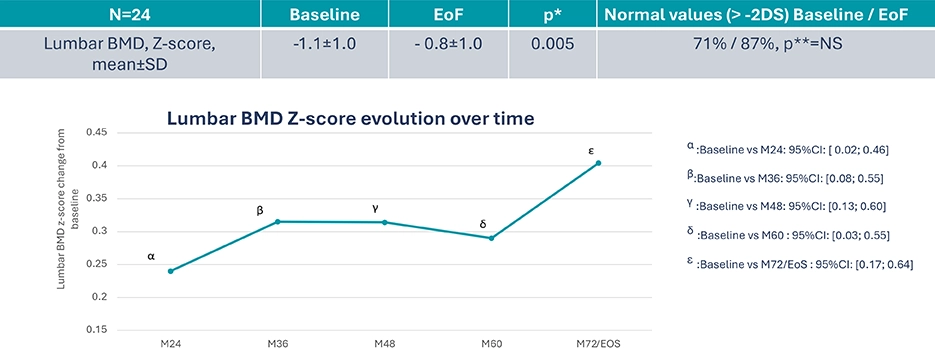
*Post hoc analysis, paired t-test
**Post hoc analysis, Mac Nemar’s test
Exploratory endpoints: Lumbar BMD in pre and post pubertal patients
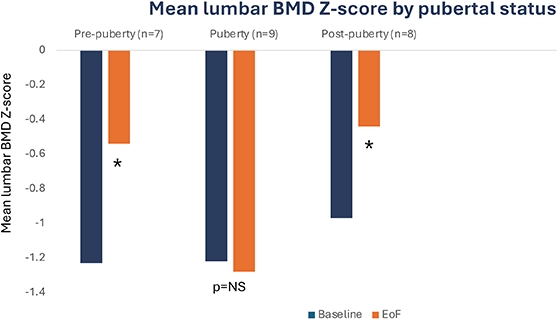
;
*Post hoc analysis, paired t-test, p<0.05
Exploratory endpoints: Quality of life (quantitative assessment at M6 and M24) and treatment acceptability about switch from SoC to ADV7103 using a VAS
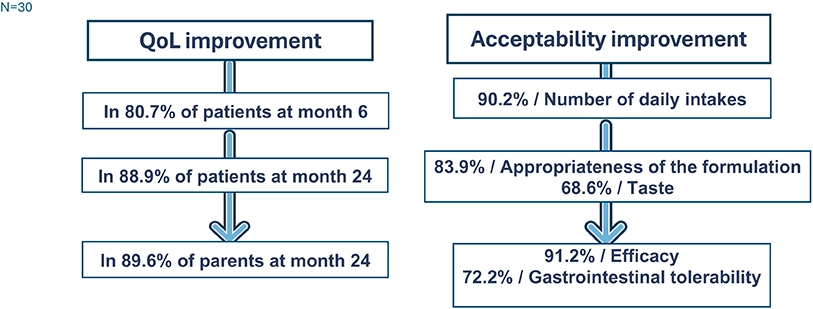
Exploratory endpoints: Quality of life (qualitative assessment at M60) following switch from SoC to ADV7103, 1-hour interviews
- Mean patients’ satisfaction score with ADV7103: 90%
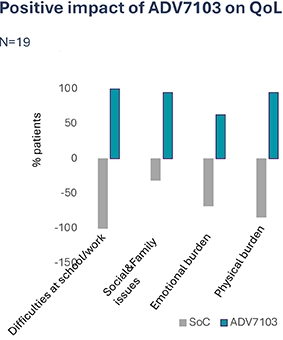
- Several QoL domains improved when treatment switched from SoC to ADV7103:
- School/work life: e.g. not interrupted/affected by burdensome number of intakes
- Social/family life: e.g. travel/holidays/social activities/family relationship easier, not thinking about managing treatment during day/night
- Emotional functioning: e.g. absence of invasive questions related to the treatment
- Physical health: e.g. reported neutral taste, absence of bad breath, absence of GI disorders, and less strong physical impacts (reported by only 16%, n=3)
- 2 available dosages: 8mEq and 24mEq

- When initiating alkalising therapy, the target starting daily dose indicated below for each age group should be used and incrementally titrated to obtain the optimal dose that provides adequate metabolic acidosis control, based on plasma bicarbonate levels
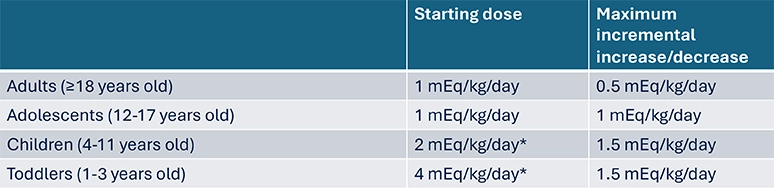
Dose is higher in infants and children due to an increase acid load subsequent to higher metabolic rate and associated higher protein intake, as well as acid generation from skeletal mineralisation6
- When switching from another alkalizing therapy, Sibnayal should be initiated at the target dose used with the previous alkalizing therapy (in mEq/kg/day) and titrated where necessary
- Dosage of Sibnayal sachets in mEq corresponds to their content in alkali, so bicarbonate plus citrate, consequently, the potassium content in mEq is the same as that of bicarbonate plus citrate
- Bicarbonate is a monovalent anion so its dose in mEq is the same as in mmole
- Citrate is a trivalent anion, so its dose in mEq is 3-fold that in mmole
- Potassium is a monovalent cation so its dose in mEq is the same as in mmole

- When switching from another alkalizing therapy, Sibnayal should be initiated at the target dose used with the previous alkalizing therapy (in mEq/kg/day) and titrated where necessary
- SoC dose is to be first converted in mEq as it is often given in mmole
- If SoC is a monovalent anion (e.g bicarbonate), the content in mEq is the same as in mmole
- If SoC is a trivalent anion (e.g citrate), the content in mEq is 3-fold that in mmole
- Then the converted alkali dose of SoC into mEq is to be given in 2 daily intatkes, 1 morning intake and 1 evening intake
- In cases where the SoC does not contain potassium, the potassium given as supplementation must be stopped as Sibnayal provides potassium in addition to alkali treatment
- The maximum dose, regardless of age group, is either 10mEq/kg/day or a total daily dose of 336 mEq, whichever is lower